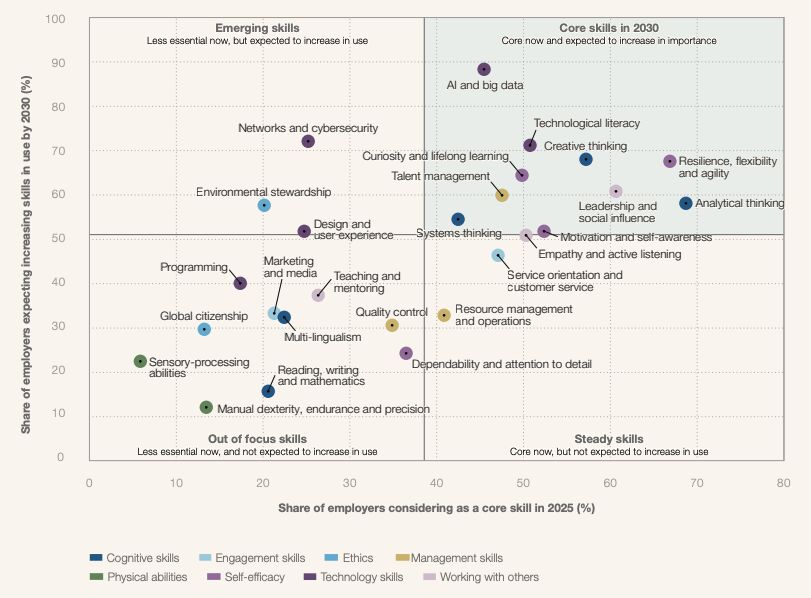
The skills that matter are changing.
We're entering a decade where skills are being redefined in real-time.
Skills are changing faster than training can follow. AI fluency and technological literacy aren't optional add-ons anymore. In healthcare, that shift is already at the bedside, in documentation, in imaging, and across operations.
Source
- World Economic Forum. Future of Jobs Report 2025. Insight Report, January 2025. ISBN 978-2-940631-90-2.
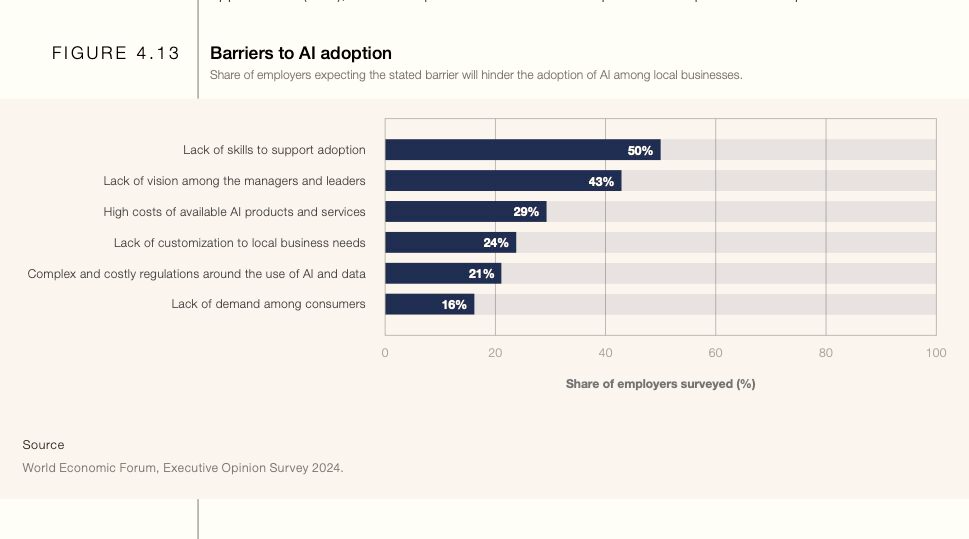
Lack of skills is the #1 barrier to AI adoption.
58% of clinicians already use AI in practice. 93% say they need more training. 32% already see patients arriving with AI-generated health information. Adoption is running ahead of competency. The gap is widening.
6 peer-reviewed papers Tap to expand
The research backs it up. Across multiple peer-reviewed studies and reviews:
Kimiafar et al. (2023)Systematic review · Front Health Inform · Clinicians lack training to use AI safely

Schubert et al. (2024)Lancet eClinicalMedicine · The case for structured AI education for clinicians
Laupichler et al. (2024)BMC Med Educ · Medical students show measurable gaps in AI literacy
Issa et al. (2024)BMC Med Educ · Competency gaps appear across roles and countries
Keren et al. (2026)JAMA · AI's deepest risk is "neverskilling" — trainees who never develop clinical expertise because AI removes the struggle that builds it
Deng et al. (2026)Lancet Primary Care · 28% of GPs already use AI but training remains ad hoc. Workforce preparedness is a patient safety issue
Sources
- World Economic Forum. Future of Jobs Report 2025.
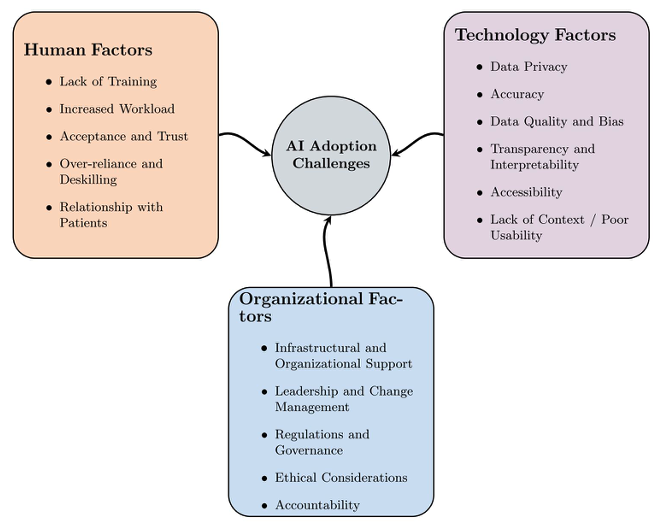
- Abdelwanis M, Simsekler MCE, Gabor AF, Sleptchenko A, Omar M. Artificial intelligence adoption challenges from healthcare providers' perspectives. Safety Science 2026. DOI: 10.1016/j.ssci.2025.107028
- Kimiafar K et al. Artificial intelligence literacy among healthcare professionals and students: A systematic review. Front Health Inform 2023; 12: 168. DOI: 10.30699/fhi.v12i0.524
- Schubert et al. AI education for clinicians. Lancet eClinicalMedicine, December 2024. DOI: 10.1016/j.eclinm.2024.102968
- Laupichler MC, Aster A, Meyerheim M et al. Medical students' AI literacy and attitudes towards AI: a cross-sectional two-center study. BMC Med Educ 24, 401 (2024). DOI: 10.1186/s12909-024-05400-7
- Issa WB, Shorbagi A, Al-Sharman A et al. Shaping the future: perspectives on the integration of Artificial Intelligence in health profession education: a multi-country survey. BMC Med Educ 24, 1166 (2024). DOI: 10.1186/s12909-024-06076-9
- Keren S et al. Promoting Clinical Expertise in the Age of AI: No Struggle, No Mastery. JAMA, 2026. DOI: 10.1001/jama.2026.6097
- Deng F et al. The mandate for clinical artificial intelligence education in primary care. Lancet Primary Care, 2026. DOI: 10.1016/j.lanprc.2026.100146
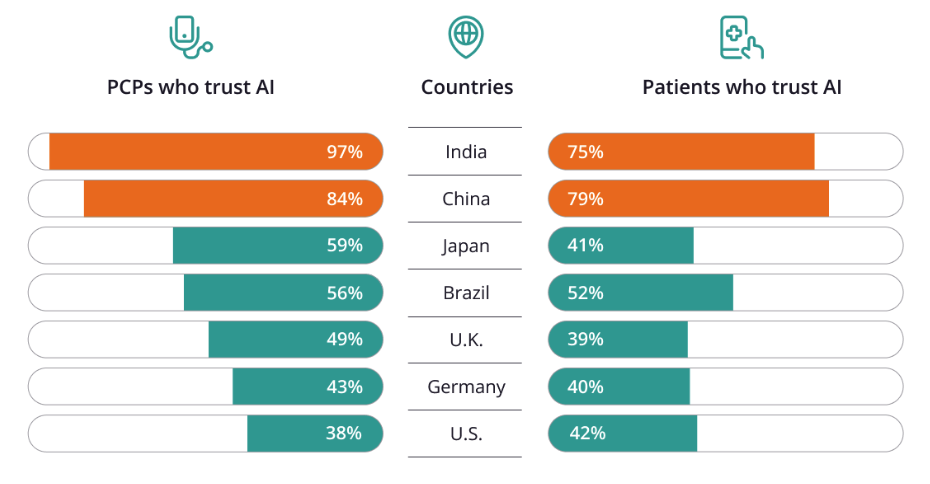
Acceptance varies. Fluency is the lever we control everywhere.
Trust in AI isn't uniform across markets. Primary-care physicians in India and China report 97% and 84% willingness to trust AI. Germany sits at 43%, the U.S. at 38%. Patient trust mirrors the same gradient, and varies sharply by task. In Germany, 87% of patients accept AI for diagnostics. That drops to 25% for triage. Meet clinicians and patients where they are. Sequence by task. Build from there.
Sources
- ZS Future of Health Survey. Base: 12,000 healthcare consumers and 1,199 PCPs across U.S., India, China, Brazil, U.K., Germany, Japan.
- Gillespie N, Lockey S, Ward T, Macdade A, Hassed G (2025). Trust, attitudes and use of artificial intelligence: A global study 2025. University of Melbourne & KPMG. DOI: 10.26188/28822919
- Baldus J et al. Patient trust in AI in radiology: task-specific analysis. Insights into Imaging 2026. DOI: 10.1186/s13244-025-02159-3
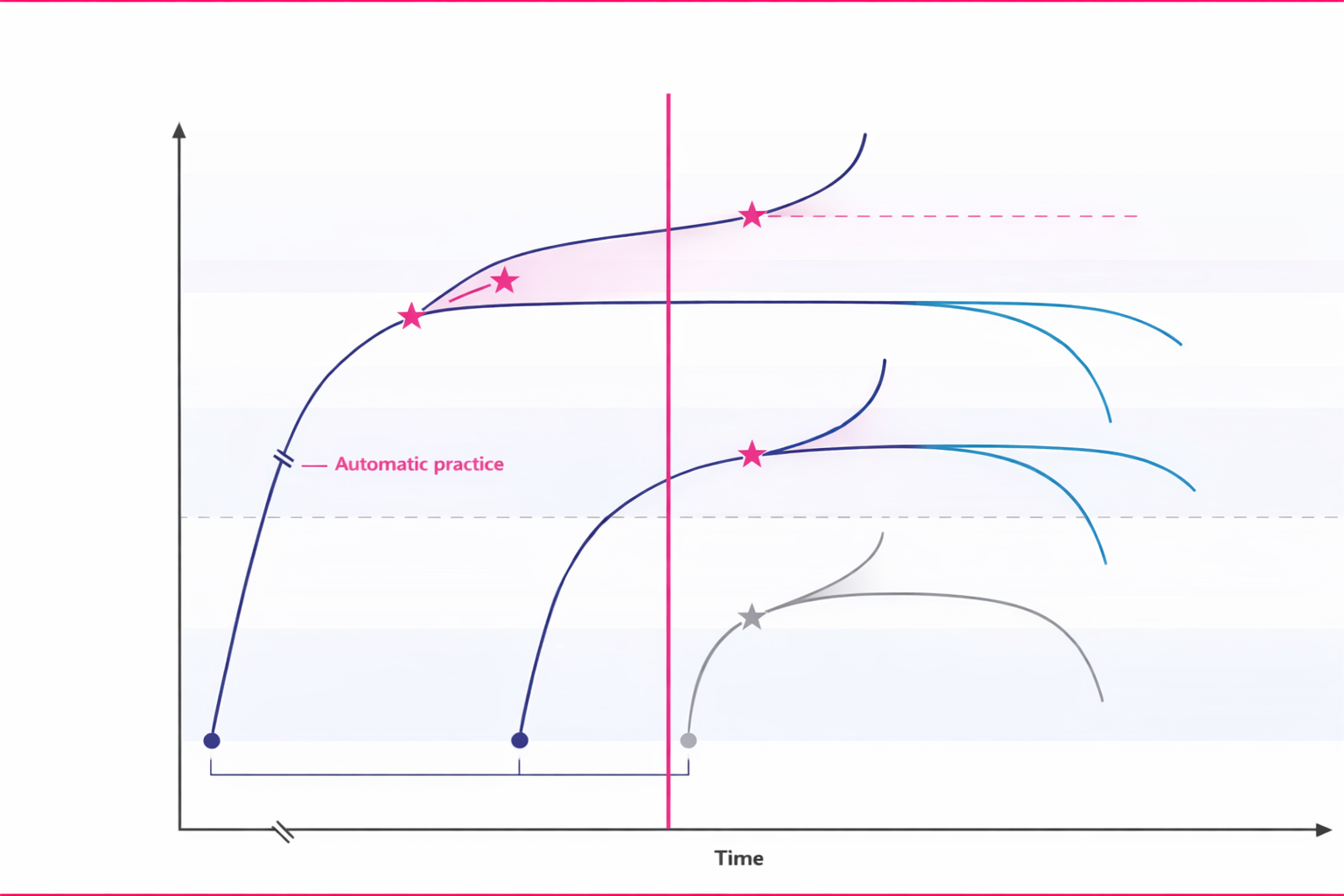
When AI arrives, performance splits three ways.
Unstructured exposure to AI isn't neutral. Clinicians who adapt actively improve. Those who rely passively on AI outputs mis-skill or deskill. The difference isn't talent. It's whether structured guidance was in place when AI arrived.
Sources
- Berzin TM et al. Preserving clinical skills in the age of AI assistance. The Lancet 2025; 406(10513): 1719.
- Abdulnour RE, Gin B, Boscardin C. Educational Strategies for Clinical Supervision of Artificial Intelligence Use. N Engl J Med 2025; 393(8): 786-797. DOI: 10.1056/NEJMra2503232
The autopilot trap is real.
A multicentre observational study of endoscopists exposed to AI in colonoscopy showed measurable deskilling. The findings: passive reliance on AI degraded human performance. After AI introduction and subsequent removal, adenoma detection rates fell by 6.0 percentage points.
"Passive reliance degrades skill. Active collaboration sharpens it."
And training alone doesn't fix it. An RCT (Succi et al., NEJM AI, 2026) enrolled physicians who completed 20 hours of structured AI literacy training. When the AI gave wrong recommendations, diagnostic accuracy still fell from 84.9% to 73.3%, a 14-point drop. Structured education is necessary. It is not sufficient without the habits to override.
The way out is structured practice, not just structured learning. Apply where it helps. Question when context is off. Document the role AI played in the decision.
Sources
- Budzyński K, Romańczyk M, Kitala D et al. Endoscopist deskilling risk after exposure to artificial intelligence in colonoscopy: a multicentre, observational study. The Lancet Gastroenterology & Hepatology 2025; 10(10): 896-903. DOI: 10.1016/S2468-1253(25)00133-5
- Succi MD et al. Effect of Erroneous Large Language Model Recommendations on Physician Diagnostic Accuracy. NEJM AI 2026. DOI: 10.1056/AIoa2501001